Updated May 2026
Surveillance after primary curative therapy for cervical cancer is recommended, although its effectiveness is not well studied. Surveillance serves several goals:
- To determine the patient's immediate response to the treatment employed
- Early recognition and prompt management of treatment-related complications
- Early detection of persistent or recurrent disease
- Collection of meaningful data regarding the efficacy of existing treatment policies and their complications so that appropriate modifications can be instituted
Surveillance Schedule
Updated consensus-based recommendations for post-treatment surveillance are as follows1-3:
- Years 1–2: every 3–4 months
- Years 3–5: every 6–12 months
- Years 5+: annually
Follow-up visits should include a thorough history and physical examination. This examination should include bimanual pelvic, rectal, and speculum exams.
After definitive radiotherapy. PET-CT is routinely performed 3–6 months post-treatment. Otherwise, in the absence of symptoms or suspicious findings, routine imaging and blood work (including tumour markers) are not recommended. However, in the following scenarios further imaging may be considered:
- Clinical suspicion of residual disease
- Residual abnormal findings on post-treatment MRI
- Progressive disease potentially amenable to salvage treatment
Fertility Sparing Surgery
In patients treated with fertility-sparing procedures (e.g., conization, radical trachelectomy), clinical surveillance should occur as outlined above or as indicated. Pelvic MRI can be considered 6 months post-treatment and annually for 2–3 years to assess local recurrence2.
While there is no high-level evidence, retrospective series support MRI's utility in detecting asymptomatic local recurrences and assessing complex postoperative anatomy4. MRI is especially helpful for evaluating the residual cervix, distinguishing between fibrosis and recurrence, and identifying parametrial or pelvic sidewall disease. Surveillance MRI is most justified in patients with tumours >2 cm, close or positive margins, or high-risk histologies2.
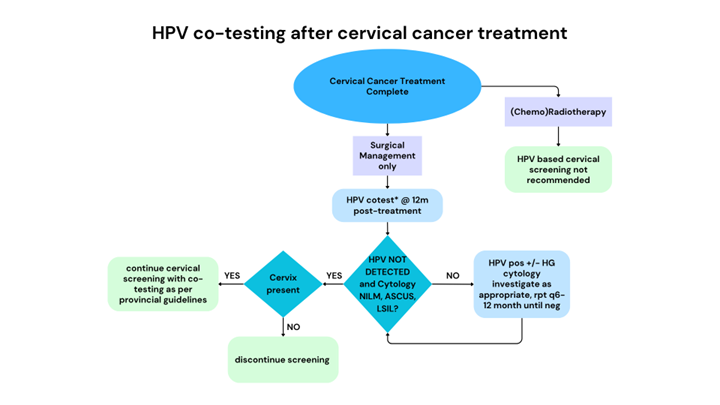
HPV co-testing after Cervical Cancer Treatment
The detection of high-risk HPV post-treatment is not associated with recurrence and may lead to unnecessary investigations. Thus, routine use of HPV testing to detect recurrence is not supported5.
Patients who have been treated with radiotherapy should not have cervicovaginal cytology as part of follow-up, as radiation-induced tissue changes compromise the reliability of cytology. For these patients, surveillance should focus on symptom review and clinical examination.
For patients treated with surgery alone, co-testing should be performed 12 months after surgical treatment. In cases of hysterectomy, co-testing should be discontinued if high-risk HPV (hrHPV) is not detected and the cytology is NILM/ASC-US/LSIL. After fertility sparing surgery, co-testing should continue as per BC Cancer cervical screening and colposcopy guidelines. Once a patient has a cervical cancer diagnosis, they are no longer recalled by the Cervix Screening Program, and it is incumbent on the oncology team to outline screening recommendation on discharge from BC Cancer.
For current recommendations, refer to the BC Cancer Cervix Screening Program and Colposcopy Guidelines:
http://www.bccancer.bc.ca/screening/health-professionals/cervix
http://www.bccancer.bc.ca/screening/Documents/Colposcopy-Guidelines.pdf
Survivorship and Management of Menopausal Hormone Therapy (MHT) Following Cervical Cancer Treatment
There is no cancer-related contraindication systemic hormone therapy after treatment for cervical or vaginal cancer. Many of these patients are young and at high risk for estrogen deprivation related morbidity6.
General Approach
Most patients will start hormone therapy after treatment completion, individualizing by symptoms, risks, and preferences.
Benefits of MHT
- Long-term beneficial impact on bone, cardiovascular and cognitive health in women with early menopause (<45 years)
- Treatment of bothersome vasomotor symptoms (hot flashes, night sweats). Patients may also notice improvement in other menopausal symptoms on MHT, such as sleep, brain fog, joint pain, mood
- Treatment of Genitourinary Syndrome of Menopause (GSM): dyspareunia, vulvovaginal dryness/discomfort and/or urinary symptoms
MHT Initiation and Duration of Treatment
- Initiation: Offer once treatment is complete and surveillance is stable.
- Duration: Often continued to ~age 51 (average natural menopause), with longer use based on individualized risk-benefit and patient preference. There is no mandatory stop time for patients who want to use MHT long-term
Prescribing MHT
Route considerations:
- Transdermal estrogen is associated with lower VTE, stroke, and hypertriglyceridemia risk vs oral; choose transdermal in higher-risk patients.
- Oral is reasonable in low-risk patients.
If the uterus is present patients require both estrogen and progesterone. If the patient has had a hysterectomy, then can use estrogen only. If endometriosis was noted in the surgical specimen post hysterectomy, then progesterone should be considered.
Options for MHT7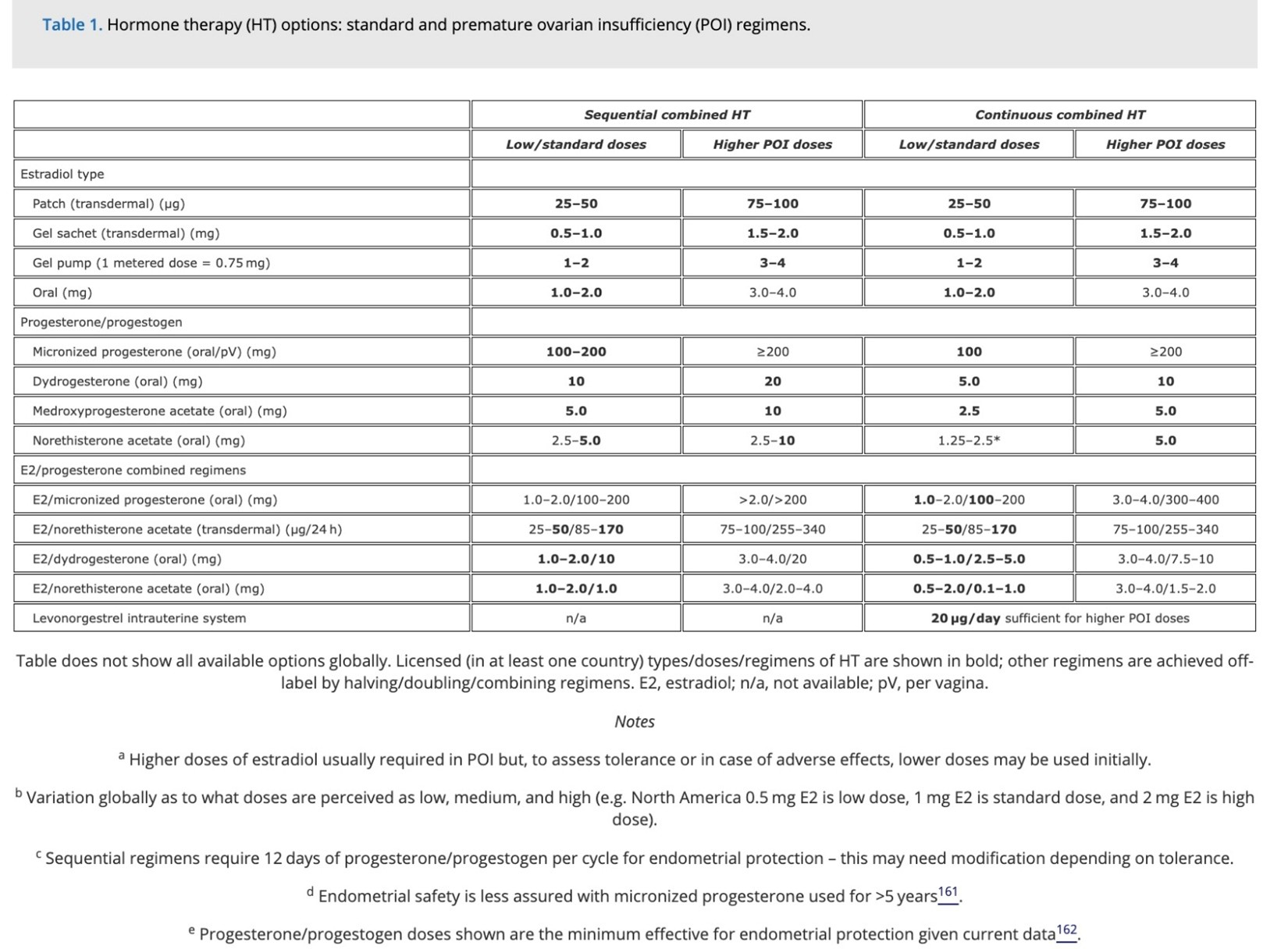
Local therapy for Genitourinary Syndrome of Menopause (GSM):
- Low-dose vaginal estrogen can be added for persistent GSM symptoms, including with systemic therapy.
- Options: Estrone 0.1% cream (Estragyn), CES cream (Premarin), Estradiol suppositories (Imvexxy 4 mcg, 10 mcg), Estradiol tablets (Vagifem 10 mcg)
- Low dose vaginal estrogen should also be considered in patients post brachytherapy to improve vaginal health
Contraindications
- Active hormone sensitive cancer or recurrence
- Unexplained vaginal bleeding
- History of thromboembolism (caution needed and topical estradiol is preferred)
Vaginal Dilators and Physiotherapy after Radiotherapy for Cervical Cancer
Radiotherapy for cervical cancer frequently results in vaginal stenosis. This condition can lead to significant morbidity, including dyspareunia, discomfort during gynecological examinations, and overall reduced quality of life. The implementation of vaginal dilators and physiotherapy can be instrumental in mitigating these adverse effects.
Vaginal Dilators
Vaginal dilators are medical devices designed to maintain vaginal patency and elasticity. They are available in various sizes and are typically composed of plastic or silicone. The primary objectives of using vaginal dilators include:
- Prevention of Vaginal Stenosis: Regular use of dilators helps to prevent the narrowing of the vaginal canal by maintaining its patency.
- Reduction of Dyspareunia: By promoting tissue flexibility and reducing fibrosis, dilators can alleviate pain during sexual intercourse.
- Facilitation of Gynecological Examinations: Dilators can make pelvic examinations more comfortable for patients by preventing stenosis.
Patients are generally advised to commence the use of vaginal dilators a few weeks post-radiotherapy. The recommended regimen typically involves using the dilators several times per week for approximately 10-15 minutes per session.
CANO Patient Education Link: https://www.cano-acio.ca/page/Patient_Education
Physiotherapy
Pelvic floor physiotherapy is another critical component of post-radiotherapy care for cervical cancer patients. A physiotherapist specializing in pelvic health can provide comprehensive management, including:
- Pelvic Floor Muscle Training: Strengthening the pelvic floor muscles can counteract the weakening effects of radiotherapy, thereby supporting the bladder, bowel, and uterus.
- Manual Therapy: Techniques such as myofascial release and trigger point therapy can be employed to alleviate pain and enhance tissue mobility.
- Patient Education: Physiotherapists can offer guidance on the correct use of vaginal dilators and develop personalized exercise programs tailored to the patient's specific needs.
To find a pelvic floor PT in BC, search through: https://bcphysio.org/find-a-physio-clinic/
Survivorship Care Responsibilities
Initial follow-up should be provided by BC Cancer medical staff. Once the patient is stable and beyond the high-risk recurrence window, follow-up care may be transitioned to the referring provider or family physician, with a clear care plan in place.
Upon discharge from oncology care:
- A summary of treatment and surveillance plan should be shared with the primary care provider.
- Education of both patient and provider regarding signs and symptoms of recurrence should be prioritized.
It is the responsibility of the oncology team and primary care provider to ensure appropriate post-treatment follow-up is arranged.
- Elit L., Kennedy E.B., Fyles A., Metser U. Follow-up for cervical cancer: a Program in Evidence-Based Care systematic review and clinical practice guideline update. Curr. Oncol. 2016;23(2):109–18. (In eng). DOI: 10.3747/co.23.2742.
- Cibula D., Raspollini M.R., Planchamp F., et al. ESGO/ESTRO/ESP Guidelines for the management of patients with cervical cancer - Update 2023. Int. J. Gynecol. Cancer 2023;33(5):649–666. (In eng). DOI: 10.1136/ijgc-2023-004429.
- National Comprehensive Cancer Network N. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Cervical Cancer (Version 4.2025). (https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf).
- Bentivegna E., Gouy S., Maulard A., Chargari C., Leary A., Morice P. Oncological outcomes after fertility-sparing surgery for cervical cancer: a systematic review. Lancet Oncol. 2016;17(6):e240–e253. (In eng). DOI: 10.1016/s1470-2045(16)30032-8.
- Aryasomayajula C., Chanana A., Tandel M., et al. The role of high-risk HPV testing in cervical cancer surveillance. Gynecol. Oncol. 2022;164(2):357–361. (In eng). DOI: 10.1016/j.ygyno.2021.11.014.
- The Hormone Therapy Position Statement of The North American Menopause Society" Advisory P. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause 2022;29(7):767–794. DOI: 10.1097/GME.0000000000002028.
- Panay N., Anderson R.A., Nappi R.E., et al. Premature ovarian insufficiency: an International Menopause Society White Paper. Climacteric 2020;23(5):426–446. DOI: 10.1080/13697137.2020.1804547.
Acknowledgements
- Dr. Andrea Neilson
- Dr. Yvette Drew
- Dr. Janice Kwon
- Dr. Hamid Raziee
- Dr. Carolyn Holloway
- Dr. Anna Tinker
- Dr. Lily Proctor
- Dr. Gina Ogilvie
- Laurie Smith
- Dr. Jennifer Pors
- Dr. Melanie Altas
- Dr. Lesa Dawson
- Dr. Amy Jamieson
- Dr. Jessica McAlpine
- Dr. Nataliya Moldovan
- Dr. Alannah Smrke
- Dr. Iwa Kong
- Dr. Shaina Lee
- Dr. Ryan Urban
- Dr. Justin McGinnis
- Sarah Buddingh Smith
- Gynecology Tumour Group

