Updated May 2026
FIGO staging of cancer of the cervix uteri (2018)
I
| Carcinoma confined strictly to the cervix (extension to corpus disregarded) |
| IA | Invasive carcinoma diagnosed only by microscopy; stromal invasion ≤5 mm depth |
– IA1
| Stromal invasion ≤3 mm depth |
| – IA2 | Stromal invasion >3 mm and ≤5 mm |
| IB | Clinically visible lesion confined to cervix or microscopic lesion >5 mm depth |
| – IB1 | Tumour <2 cm in greatest dimension |
| – IB2 | Tumour ≥2 cm and <4 cm |
| – IB3 | Tumour ≥4 cm |
| II | Tumour invades beyond uterus but not to pelvic wall or lower third of vagina |
| IIA | Tumour invades upper two-thirds of vagina without parametrial involvement |
| – IIA1 | Tumour <4 cm |
| – IIA2 | Tumour ≥4 cm |
| IIB | Tumour with parametrial involvement but not up to pelvic wall |
| III | Tumour involves lower third of vagina and/or pelvic wall and/or causes hydronephrosis or non-functioning kidney or involves lymph nodes |
| – IIIA | Involves lower third of vagina, no pelvic wall extension |
– IIIB
| Extension to pelvic wall and/or hydronephrosis or non-functioning kidney |
| – IIIC | Involves lymph nodes (any tumour size) |
| – IIIC1(r/p) | Pelvic lymph node involvement (radiologic [r] or pathologic [p]) |
– IIIC2(r/p)
| Para-aortic lymph node involvement (± pelvic nodes), radiologic or pathologic |
| IVA | Tumour invades mucosa of bladder or rectum and/or extends beyond true pelvis |
| IVB | Distant metastasis (e.g., lungs, liver, bone, inguinal nodes) |
Footnotes:
- Stage IB is now subdivided based on lesion size: IB1 (<2 cm), IB2 (≥2 cm and <4 cm), IB3 (≥4 cm).
- Stage IIIC is a new classification based on imaging (r) or pathology (p) identifying nodal involvement.
- Hydronephrosis must be due to tumour to assign Stage IIIB.
- Distant metastases to inguinal nodes are included in Stage IVB.
Cervical Cancer TNM staging – AJCC Version 92
Primary Tumour (T)
TX
|
| Primary tumour cannot be assessed |
T0
|
| No evidence of primary tumour |
| T1 | I | Carcinoma is strictly confined to the cervix (extension to the corpus should be disregarded) |
T1a
| IA | Invasive carcinoma diagnosed only by microscopy with max depth of invasion ≤5 mm
|
| T1a1 | IA1 | Measured stromal invasion ≤3 mm
|
| T1a2 | IA2 | Measured stromal invasion >3 mm and ≤5 mm |
| T1b | IB | Invasive carcinoma >5 mm in depth, limited to cervix uteri |
| T1b1 | IB1 | Invasive carcinoma >5 mm depth, ≤2 cm greatest dimension |
| T1b2 | IB2 | Invasive carcinoma >2 cm and ≤4 cm |
| T1b3 | IB3 | Invasive carcinoma >4 cm |
| T2 | II | Carcinoma invades beyond uterus but not lower third of vagina or pelvic wall |
| T2a | IIA | Upper two-thirds of vagina involved, no parametrial invasion |
| T2a1 | IIA1 | Invasive carcinoma ≤4 cm |
| T2a2 | IIA2 | Invasive carcinoma >4 cm |
| T2b | IIB | With parametrial invasion but not to pelvic wall |
| T3 | III | Involves lower third of vagina and/or pelvic wall and/or causes hydronephrosis |
| T3a | IIIA | Involves lower third of vagina, no extension to pelvic wall |
| T3b | IIIB
| Extension to pelvic wall and/or hydronephrosis |
| T4 | IVA | Involves mucosa of bladder or rectum, or adjacent organs |
Regional Lymph Nodes (N)
NX
|
| Regional lymph nodes cannot be assessed |
| N0 |
| No regional lymph node metastasis |
| N0(i+) | | Isolated tumour cells ≤0.2 mm or ≤200 cells in one section |
| N1 | IIIC1 | Metastasis to pelvic lymph nodes only |
| N1mi | IIIC1 | Metastasis >0.2 mm and ≤2.0 mm to pelvic lymph nodes |
| N1a | IIIC1 | Metastasis >2.0 mm to pelvic lymph nodes |
| N2 | IIIC2 | Metastasis to para-aortic lymph nodes ± pelvic nodes |
| N2mi | IIIC2 | Metastasis >0.2 mm and ≤2.0 mm to para-aortic nodes |
| N2a | IIIC2 | Metastasis >2.0 mm to para-aortic nodes |
| M0 |
| No distant metastasis |
| cM1 | IVB | Distant metastasis (e.g., lung, liver, bone, inguinal nodes) |
| pM1 | IVB | Microscopically confirmed distant metastasis |
| I | T1 | N0 | M0 |
| IA | T1a | N0 | M0 |
IA1
| T1a1 | N0 | M0 |
| IA2 | T1a2 | N0 | M0 |
| IB | T1b | N0 | M0 |
| IB1 | T1b1 | N0 | M0 |
| IB2 | T1b2 | N0 | M0 |
| IB3 | T1b3 | N0 | M0 |
| II | T2 | N0 | M0
|
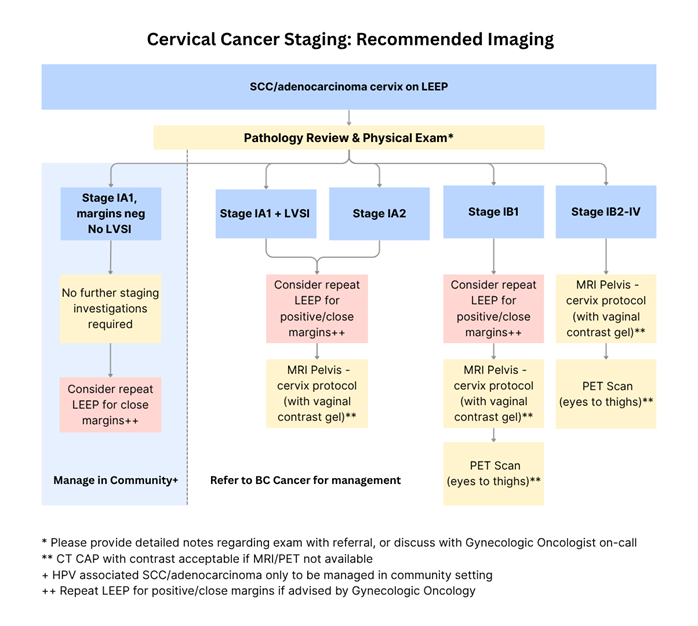
Following biopsy confirmation of carcinoma of the cervix, history and physical examination and the following staging investigations should be done:
Lab studies: CBC, differential, BUN and creatinine, liver function tests and β-HCG in pre-menopausal patients, as indicated.
Radiological studies: MRI pelvis with vaginal contrast (cervix protocol) for all cases referred to BC Cancer. PET-CT scan for patients with suspected stage IB1 disease or higher. CT scan of the chest-abdomen-pelvis can be done if PET scan is not available.
Examination under anesthesia (EUA): if necessary, to assess primary tumour volume and extent.
- Bhatla N., Aoki D., Sharma D.N., Sankaranarayanan R. Cancer of the cervix uteri. International Journal of Gynecology & Obstetrics 2018;143(S2):22–36. DOI:
https://doi.org/10.1002/ijgo.12611.
- Olawaiye A.B., Baker T.P., Washington M.K., Mutch D.G. The new (Version 9) American Joint Committee on Cancer tumor, node, metastasis staging for cervical cancer. CA: A Cancer Journal for Clinicians 2021;71(4):287–298. DOI:
https://doi.org/10.3322/caac.21663

