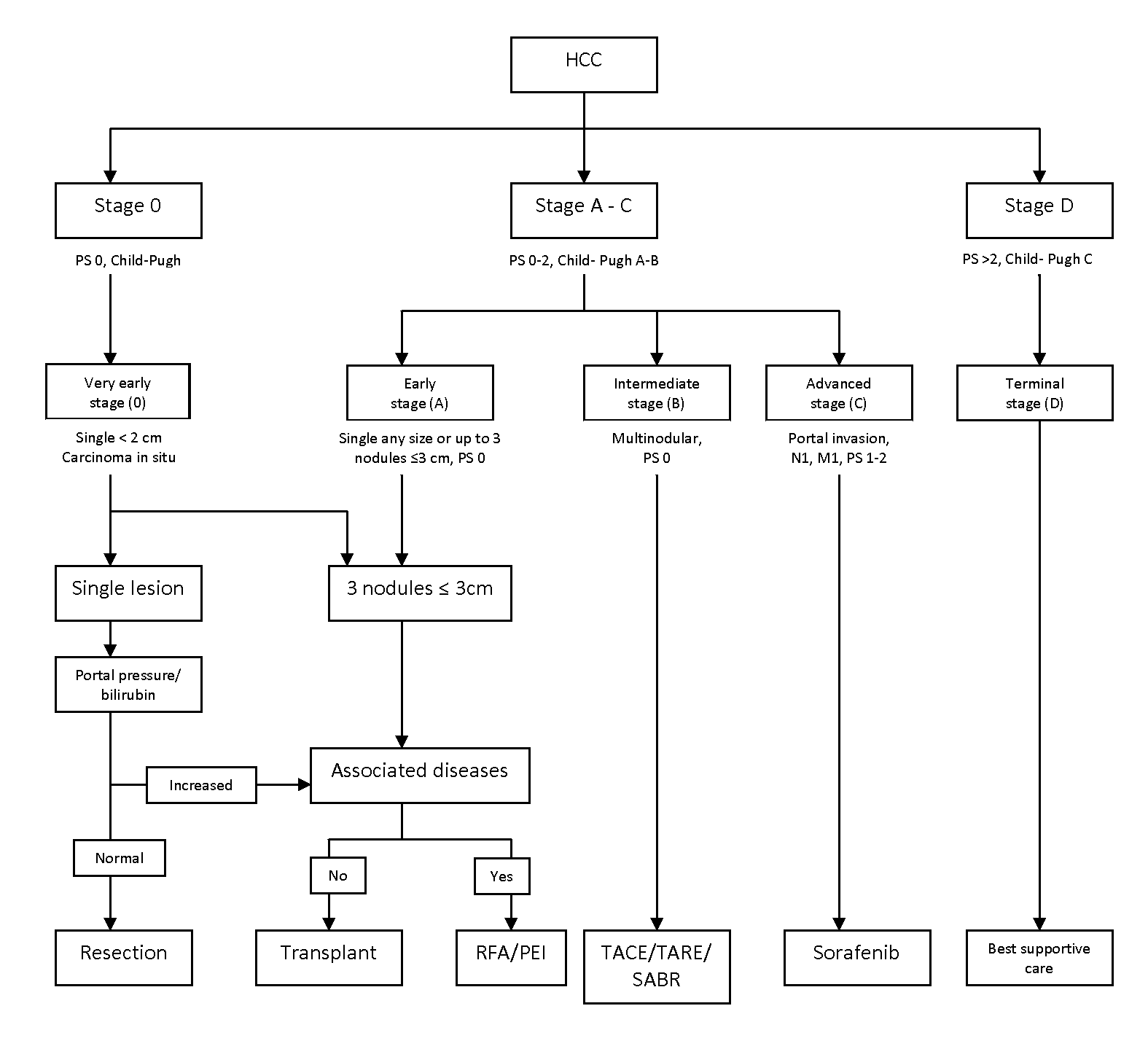
The Barcelona Clinic Liver Cancer (BCLC) staging system is a widely recognized staging system to help determine the appropriate treatments for patients with any stage of HCC.
-
Patients must
have ECOG Performance Status 0 and Child-Pugh A liver function
-
Tumours must be less than 2 cm and confined to one lobe of the liver, with absence of vascular invasion and extra-hepatic disease, and complete removal of the tumour with a margin of greater than 1 cm is anticipated
-
Recommended treatment is ablation or resection if ablation is not possible (see above)
-
There is no role adjuvant chemotherapy or radiotherapy
- Patients must have ECOG Performance Status 0 and Child-Pugh A liver function
- Tumours must be confined to one lobe of the liver or up to three nodules all less than 3 cm, with absence of vascular invasion and extra-hepatic disease, and complete removal of the tumour with a margin of greater than 1 cm is anticipated
- A solitary tumour of any size may be considered for resection provided the liver function is satisfactory and there is an adequate future liver remnant
- Recommended treatment is surgical with resection or in certain circumstances liver transplantation. Alternatively, local treatment with radiofrequency ablation (RFA) or percutaneous ethanol injection (PEI) can be used for patients with tumours less than 3 cm that are not surgical/transplant candidates or refuse surgery
- Patients must have ECOG Performance Status 0, Child-Pugh A liver function or selected patients with Child-Pugh B liver function and have adequate renal (liver?) function
- Tumours are multinodular with absence of extra-hepatic disease, with patency of the main portal vein
- Recommended treatment is locoregional with trans-arterial chemo-embolization (TACE) or trans-arterial radio-embolization (TARE - see
UGIYTT)
- Stereotactic Ablative Radiotherapy (SABR) is also an option
- No role for adjuvant chemotherapy, although clinical trials are underway
- Patients being considered for systemic treatment must have ECOG Performance Status 0, 1 or 2 and Child-Pugh A liver function
- These patients with HCC are ineligible for, or have progressed after, surgical or locoregional therapy
- Palliative systemic therapy may be given to help improve symptoms and quality of life, and extend survival in appropriately selected patients
- Currently approved systemic agents for HCC include: sorafenib (see
UGISORAF) and doxorubicin (see
GIA)
- Consider treatment on a clinical trial, if available
- Palliative radiotherapy for pain control
- Symptom management, best supportive care, and involvement of palliative care services as indicated by patient’s clinical status
- Patients with ECOG Performance Status greater than 2 and/or Child-Pugh C liver function
- Palliative chemotherapy may adversely affect outcome
- Palliative radiotherapy for pain control
- Symptom management, best supportive care, and involvement of palliative care services highly recommended

