View the images and select the correct diagnosis from the list below.
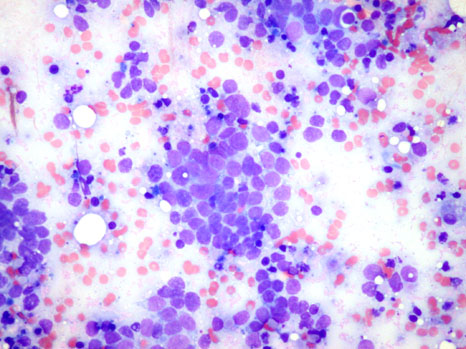
FNA from a 1.5 cm firm nodule overlying the left parotid gland from an 81-year-old woman with a remote history of basal cell carcinoma:
Select one of the following:
You answered: Lymphoma
Sorry, that is Incorrect
The correct diagnosis is: Merkel cell carcinoma
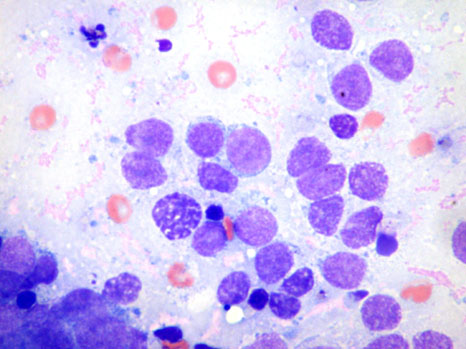
- Poorly cohesive population of small blue cells, uniform in appearance. Some clustering may be seen
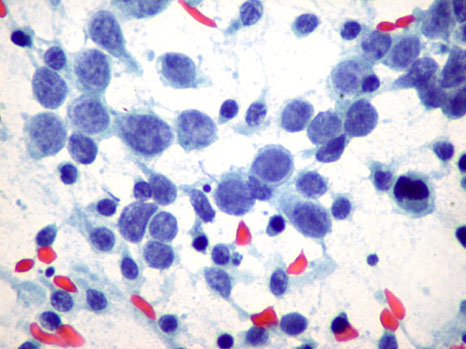
- High N/C ratios, rounded nuclei, powdery chromatin (best appreciated on fixed specimens), inconspicuous nucleoli, scant cytoplasm
- "Blue buttons" (perinuclear cytoplasmic aggregates of intermediate filaments) in cytoplasm, but not specific and is also seen in small cell carcinoma of the lung
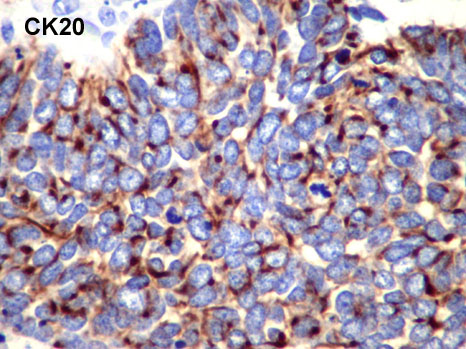
- Immunohistochemistry shows characteristic perinuclear dot-like positivity for CK20, positive for neurofilaments, negative for TTF-1 and CK7 (useful in distinction from small cell carcinoma of lung). It is also negative for LCA (distinction from lymphoma)
- This is consistent with a diagnosis of Merkel Cell Carcinoma
- Merkel cell carcinoma is a rare primary neuroendocrine carcinoma of the skin
- Most occur in the head and neck area or buttocks of elderly patients
- Clinically, this tumour is nodular with a reddish or violaceous hue, centred in the dermis.
- They are usually locally agressive and can metastasize
- Treatment involves wide resection of the primary site and regional lymph node dissection; radiation therapy can be used as an adjunct, and chemotherapy has been employed for metastatic tumours
- The major differential diagnoses are small cell carcinoma of the lung and malignant lymphoma
- Merkel cell carcinoma cells are more uniform (with no irregular or spindle-shaped cells), with minimal moulding, and show a more dispersed cell pattern when compared to small cell carcinoma of the lung
- Presence of true tissue aggregates and lack of lymphoglandular bodies aid in differentiating Merkel cell carcinoma from malignant lymphoma
- Basal cell carcinomas typically show large tight clusters of atypical basaloid cells, with no nuclear moulding. Cells characteristically palisade at the periphery on tissue histology
Back to images
Histology
- DeMay RM. The Art & Science of Cytopathology. Chicago: ASCP Press, 1996; 605, 630-1.
- Rosai J. Ackerman's Surgical Pathology. Mosby, 8th Edition, 1996; 166-8.
You answered: Merkel cell carcinoma
Correct!!
- Poorly cohesive population of small blue cells, uniform in appearance. Some clustering may be seen
- High N/C ratios, rounded nuclei, powdery chromatin (best appreciated on fixed specimens), inconspicuous nucleoli, scant cytoplasm
- "Blue buttons" (perinuclear cytoplasmic aggregates of intermediate filaments) in cytoplasm, but not specific and is also seen in small cell carcinoma of the lung
- Immunohistochemistry shows characteristic perinuclear dot-like positivity for CK20, positive for neurofilaments, negative for TTF-1 and CK7 (useful in distinction from small cell carcinoma of lung). It is also negative for LCA (distinction from lymphoma)
- This is consistent with a diagnosis of Merkel Cell Carcinoma
- Merkel cell carcinoma is a rare primary neuroendocrine carcinoma of the skin
- Most occur in the head and neck area or buttocks of elderly patients
- Clinically, this tumour is nodular with a reddish or violaceous hue, centred in the dermis.
- They are usually locally agressive and can metastasize
- Treatment involves wide resection of the primary site and regional lymph node dissection; radiation therapy can be used as an adjunct, and chemotherapy has been employed for metastatic tumours
- The major differential diagnoses are small cell carcinoma of the lung and malignant lymphoma
- Merkel cell carcinoma cells are more uniform (with no irregular or spindle-shaped cells), with minimal moulding, and show a more dispersed cell pattern when compared to small cell carcinoma of the lung
- Presence of true tissue aggregates and lack of lymphoglandular bodies aid in differentiating Merkel cell carcinoma from malignant lymphoma
- Basal cell carcinomas typically show large tight clusters of atypical basaloid cells, with no nuclear moulding. Cells characteristically palisade at the periphery on tissue histology
Back to images
- DeMay RM. The Art & Science of Cytopathology. Chicago: ASCP Press, 1996; 605, 630-1.
- Rosai J. Ackerman's Surgical Pathology. Mosby, 8th Edition, 1996; 166-8.
You answered: Basal cell carcinoma
Sorry, that is Incorrect
The correct diagnosis is: Merkel cell carcinoma
- Poorly cohesive population of small blue cells, uniform in appearance. Some clustering may be seen
- High N/C ratios, rounded nuclei, powdery chromatin (best appreciated on fixed specimens), inconspicuous nucleoli, scant cytoplasm
- "Blue buttons" (perinuclear cytoplasmic aggregates of intermediate filaments) in cytoplasm, but not specific and is also seen in small cell carcinoma of the lung
- Immunohistochemistry shows characteristic perinuclear dot-like positivity for CK20, positive for neurofilaments, negative for TTF-1 and CK7 (useful in distinction from small cell carcinoma of lung). It is also negative for LCA (distinction from lymphoma)
- This is consistent with a diagnosis of Merkel Cell Carcinoma
- Merkel cell carcinoma is a rare primary neuroendocrine carcinoma of the skin
- Most occur in the head and neck area or buttocks of elderly patients
- Clinically, this tumour is nodular with a reddish or violaceous hue, centred in the dermis.
- They are usually locally agressive and can metastasize
- Treatment involves wide resection of the primary site and regional lymph node dissection; radiation therapy can be used as an adjunct, and chemotherapy has been employed for metastatic tumours
- The major differential diagnoses are small cell carcinoma of the lung and malignant lymphoma
- Merkel cell carcinoma cells are more uniform (with no irregular or spindle-shaped cells), with minimal moulding, and show a more dispersed cell pattern when compared to small cell carcinoma of the lung
- Presence of true tissue aggregates and lack of lymphoglandular bodies aid in differentiating Merkel cell carcinoma from malignant lymphoma
- Basal cell carcinomas typically show large tight clusters of atypical basaloid cells, with no nuclear moulding. Cells characteristically palisade at the periphery on tissue histology
Back to images
- DeMay RM. The Art & Science of Cytopathology. Chicago: ASCP Press, 1996; 605, 630-1.
- Rosai J. Ackerman's Surgical Pathology. Mosby, 8th Edition, 1996; 166-8.
From the Cytopathology files of BC Cancer
Submitted by: Carol Lee, MD and Tom Thomson, MD

